Repeated tibial lengthening as a stage of locomotor reconstruction in achondroplasia patients
Views: 962
Russian Ilizarov Scientific Center for Restorative Traumatology and Orthopaedics, Kurgan, Russia
Objective To show that some achondroplasia cases of surgical locomotor reconstruction require repeated tibial lengthening to achieve optimal anthropometric parameters and review dynamics in reparative osteogenesis during repeated tibial lengthening using optical densitometry. Material and methods A group of patients who underwent double tibial lengthening included 25 achondroplasia and hypochondroplasia patients who underwent treatment at the Russian Ilizarov Scientific Centre “Restorative Traumatology and Orthopaedics” from 2000 to 2013. Results Review of dynamics in reparative osteogenesis revealed no specific course of the procedure. Conclusions Medical, ergonomic and esthetic aspects of achondroplasia treatment can partially be addressed by approaching anthropometric parameters to the biomechanical, ergonomic and esthetic standards through repeated lengthening of lower limb segments.
Keywords: achondroplasia, limb lengthening, ergonomics, tibial lengthening, anthropometry
INTRODUCTION
Rehabilitation of patients with achondroplasia can be considered as one of the unique forms of treatment available in orthopaedic surgery with extensive multi- staged operative interventions aimed at reconstruction of locomotor system.
The usage of public transport, industrial and house- hold equipment, occupational safety and health rules are known to impose high human requirements including ergonomic needs [1, 2]. Non-standard anthropometric measurements may interfere with everyday physical activity and overall quality of life.
The ergonomic aspects of locomotor reconstruction seek to approximate the key anthropometric human param- eters to some ergonomic standards of living environment. For this a number of anthropometric measurements needs to be corrected and lower limbs to be lengthened.
Objectives To show that some achondroplasia cases of surgical locomotor reconstruction require repeated tibial lengthening to achieve optimal anthropometric parameters and review dynamics in reparative osteogen- esis during repeated tibial lengthening using optical densitometry.
MATERIAL AND METHODS
A group of patients who underwent double tibial length- ening included 25 achondroplasia and hypochondroplasia patients who underwent treatment at the Russian Ilizarov Scientific Centre “Restorative Traumatology and Orthopae- dics” (RISC “RTO”) from 2000 to 2013. Total 50 tibiae were elongated. The average age at the time of index opera- tion was 8.3 ± 1.2 years. Unifocal tibial lengthening was produced for 17 patients due to a small length of the segment being lengthened in children aged 6 to 8 years. Repeated tibial lengthening was commenced approximately one year and more after completion of the first stage (1.8 ± 0.7 years) with the average age of the patients being 10.1 ± 2.7 years.
Evaluation of intersegmental proportions between the torso and free limbs is important from clinical point of view. The coefficient of proportionality (CP) was used in our work and expressed as a percentage meas-
ured with the formula below [3],
where L1 – total height; L2 – sitting height with normal CP measuring 87 to 92 %.
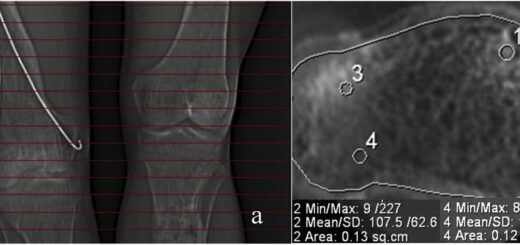
Dynamics in reparative osteogenesis was evaluated indirectly through measuring mineralisation at different parts of the segment being elongated with optical densi- tometry using digital and analog radiographs of the segment and Hi-Scene software developed at RISC “RTO”. Densitometric calculations showed how active the reparation was and also revealed structural features of the distractional regenerate bone. Optical density measurements were produced with radiographic images to evaluate mineralization in the tibial shaft and proxi- mal regenerate bone.
Klimov О.V., Aranovich А.М. Repeated tibial lengthening as a stage of locomotor reconstruction in achondroplasia patients.
Genij Ortopedii. 2017. T. 23. No 4. pp. 401-404. DOI 10.18019/1028-4427-2017-23-4-401-404. (In Russian)
RESULTS AND DISCUSSION
Although multiple lengthening procedures were per- formed for locomotor reconstruction of achondroplasia patients they were shown to be incapable to get jobs involving a lot of standing and moving, heavy lifting, associated with heavy occupational workload. They were more likely to experience different careers such as drivers, operators. Driving skills were also important for recreational and everyday activities.
These aspects of the interaction among human and other elements of a system are studied by ergonomics aimed at creating and maintaining a healthy and safe working, domestic and recreational environment. Pursu- ant to the first principle of ergonomics, workplace equipment and furniture which is appropriate and suita- ble for the work being done should be provided to assist at least 90 % of staff with the performance of work. Design technologies consider anthropometric data cor- responding to the 5th and 95th percentiles. Anthropomet- ric data of maximum longitudinal, transverse and ante- riorposterior body dimensions are considered when cal- culating minimal working area.
The second principle of ergonomics considers an- thropometric data of minimum longitudinal, transverse and anteriorposterior body dimensions when calculating clearance, reach and adjustability.
While ergonomics deals with the efficient organisation of the relationships between man and his environment we can consider anthropometric data corresponding to the 5th percentile in females for correction of anthropometric val- ues in achondroplasia patients. In this case it would be the anthropometric threshold proceeding from ergonomic principles of building up the structure and functional pa- rameters of objective-spatial environment [4].
The table below presents figures closely matching with such an important anthropometric value as sitting height, so we can conclude that social adaptation of achondroplasia patients would refer to anthropometric data of the 5th percentile female. The threshold value is considered when designing the majority of consumer products, living and working environment (Table 1) [5].
Table 1
Anthropometric measurements of normal females and achondroplasia patients (mm)
| Parts of the body | Normal female | Achondroplasia patients* | |
| 5th percentile | females | males | |
| Length of: | |||
| trunk | 150.8 | 124.5/-26.3 | 127.8/-23.0 |
| arm | 65.1 | 50.1/-15.0 | 55.1/-10 |
| leg | 78.6 | 43.6/-35.0 | 42.3/-36.3 |
| humerus | 27.7 | 20.2/-7.5 | 22.2/-5.5 |
| forearm | 21.0 | 16.3 | 17.9 |
| foot | 22.1 | 20.0 | 21.3 |
| Sitting height | 81.2 | 80.9/-0.3 | 85.5/+4.3 |
* – Authors’ measurements.
Therefore, the tactics of treatment to be performed for achondroplasia patients can shortly be described as limb lengthening, deformity correction maintaining the function. Our experience showed that average body proportions and longitudinal dimensions cannot be pro- vided in achondroplasia adults using current methods. As shown above, based on the current ergonomic stand- ards of social environment comfortable working, recrea- tional conditions are calculated with reference to mini- mal dimensions of the 5th percentile female that is a well-proportioned person with a stature of at least 150 cm. And from ergonomic point of view this is a minimal standard to strive for. However, the standard can be achieved with double tibial lengthening that is essential for most of the cases.
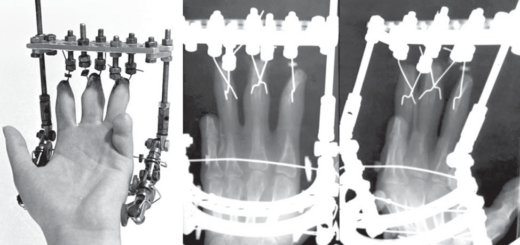
The repeated leg lengthening procedure and postop- erative care are mostly similar to those performed at index surgery. There are some specific features about the second tibial lengthening including the absence of redundantly long soft tissues with less extension capa- bilities, presence of scars from the previous surgery, some clinical and functional consequenc- es/complications from the previous procedure that might have affected the final outcome.
Depending on an interval between the index and re- peated procedure preoperative radiographs showed in- creased optical density of the bone, discontinuous in- tramedullary canal, as well as remaining signs of perios- teal reaction with thickened portions of the new bone or cortical bone defects (Table 2).
Table 2
Timing dynamics in radiological manifestations follow- ing index tibial lengthening
| Follow-up | ||||
| 1
month |
1
year |
2
years |
> 2
years |
|
| Increased optical density of the bone | 100 | 75 | 25 | 0 |
| Continuous intrame- dullary canal | 100 | 35 | 8 | 0 |
| Periosteal reaction | 100 | 45 | 12 | 5 |
| Periosteal bone defect | 50 | 50 | 10 | 2 |
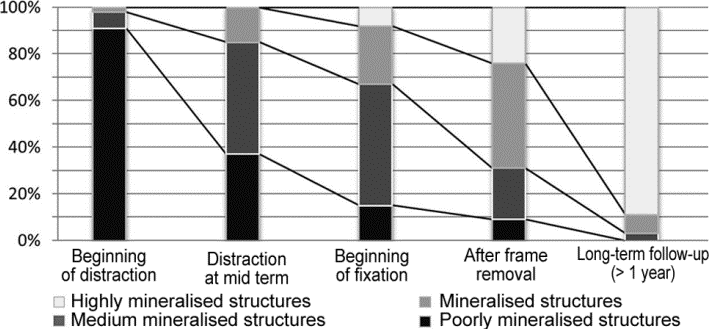
Figure 1 shows timing dynamics in reparative osteo- genesis during repeated tibial lengthening and indicates to correlations of structures with various density that changes in an inversed manner, as well as a staged pro- cess that can require correction of distraction rate or frame removal.
Fig. 1 Histogram showing structures distributed at the proximal lengthening site with regard to an extent of mineral- isation at the repeated tibial lengthening
Restructuring of the new bone is complete two years and more than two years following frame removal. The new bone structure appears normal with intramedullary canal continuity completely restored and correlation of tissues with different mineral density being typical for normal bone.
Overall dynamics in optical density of the bone and the regenerate is presented in Figure 2. The diagram shows the density of parental bone decreasing throughout the length- ening period to the beginning of fixation with the density of the regenerate bone increasing over the period.
Optical density of the distractional regenerate bone demonstrated greater values as compared to those of the
parental bone due to osteoporosis of the parental bone and absence of intramedullary canal in the regenerate bone. Absence of intramedullary canal suggested ho- mogenous regenerate structure through the bone result- ing in an overall increase in the optical density. The values were shown to change sharply with concomitant increase in the density of both the regenerate and the parental bones following the removal of external fixator. Further on, the optical density had a tendency to de- crease with intramedullary canal being formed in the new bone. There were similar optical density measure- ments throughout the whole length of the bone upon completion of restructuring processes.
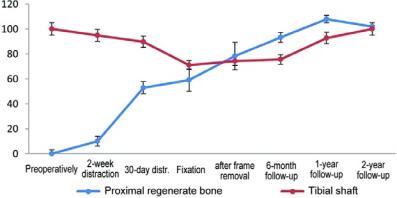
Fig. 2 Dynamics in optical density of the proximal regenerate bone and tibial shaft measured with radiographs of tibia during repeated lengthening procedure
CONCLUSIONS
The findings showed similar radiological manifestations of reparative osteogenesis in the proximal tibia during re- peated tibial lengthening and at the index surgery of tibial lengthening performed for achondroplasia patients. Such factors as osteotomy level, a contact area of bone fragments, a number of bone debris, latency period and distraction rate have a significant impact on reparative osteogenesis.
Densitometric study of bone regeneration showed more active osteogenesis in the proximal regenerate
portions. Thus, the proximal bone was found to provide more favourable conditions for reparative processes. In our opinion, there are two reasons for this, the first, re- dundant soft tissues, the second, better blood supply ensured by the proximal parts of the limbs.
Therefore, repeated tibial lengthening can be per- formed in some clinical instances in the absence of con- traindications to achieve ergonomically substantiated outcomes.
REFERENCES
- Aranovich A.M., Klimov O.V., Novikov K.I. Reabilitatsiia patsientov s nizkim rostom [Rehabilitation of patients with low stature]. Genij Ortop., 2011, no. 2, pp. 15-20. (In Russ.)
- Okuno A. Current status of diagnosis and treatment of growth retardation. Hokkaido Igaku Zasshi, 1996, vol. 71, no 2, pp. 145-150.
- Il’inich V.I., ed. Fizicheskaia kul’tura studenta: uchebnik [Physical culture of a student: a manual]. M., Gardariki, 2000, 448 p. (In Russ.)
- Munipov V.M. Ergonomika: chelovekoorientirovannoe proektirovanie tekhniki, programmnykh sredstv i sredy: uchebnik dlia studentov vuzov [Ergonomics: human-oriented design of equipment, software and environment: a textbook for students of higher education institutions]. M., Logos, 2001, 356 p. (In Russ.)
- Runge V.F. Ergonomika i oborudovanie inter’era: ucheb. posobie [Ergonomics and interior equipment: a text- book]. M., Arkhitektura-S, 2004, 160 p. (In Russ.)
Received: 12.07.2017
Information about the authors:
- Oleg V. Klimov, M.D., Ph.D., Russian Ilizarov Scientific Centre for Restorative Traumatology and Orthopaedics of the RF Ministry of Health, Kurgan, Department of Traumatology and Orthopaedics No 14, traumatologist- orthopedist of the Highest Category
- Anna M. Aranovich, M.D., Ph.D., Professor, Honored Physician of Russia, Russian Ilizarov Scientific Centre for Restorative Traumatology and Orthopaedics of the RF Ministry of Health, Kurgan, Head of Department of Trauma- tology and Orthopaedics No 17