Myotopography in Tibial Lengthening

Views: 926
COPYRIGHT 2018 © BY THE ARCHIVES OF BONE AND JOINT SURGERY
TECHNICAL NOTE
Myotopography in Tibial Lengthening
Konstantin Igorevich Novikov, PhD; Oleg Vladimirovich Klimov, MD; Koushik Narayan Subramanyam, MS (Ortho), MRCSEd; Andrey Sergeevich Neretin, MD; Olga Stepanovna Novikova, MD
Research performed at Russian Ilizarov Scientific Centre for Restorative Traumatology and Orthopaedics, Kurgan, Russia
Received: 11 June 2017 Accepted: 23 September 2017
Abstract
Limb lengthening by Ilizarov lengthens not just the long bone, but also the soft tissues too. Damage of the muscles during corticotomy and their stretching during distraction play a crucial role in occurrence of complications and final limb function. We present here a systematic codified nomenclature system of each muscle summarising all the influence that corticotomy and distraction have the particular muscle and demonstrate the same in the setting of tibial lengthening. This scheme helps the surgeon easily recollect what all muscles are involved in what all ways in each level of corticotomy thus enabling him to watch out for complications thereof and monitor and accordingly modify the limb lengthening process.
Level of evidence: V
Keywords: Distraction osteogenesis, Ilizarov, Myotopography, Tibial lengthening
Introduction
E
xternal fixation is related with high chances of pin tract infections which in turn is influenced by the location of the pin or wires in relation to
the muscles that cause motion of nearby joints(1). The science of Ilizarov is associated with various difficulties, obstacles and complications and the way to prevent them is strict adherence to technical details(2). The success lengthening of long bone is determined by its influence on the muscles that determine the movement of the adjacent joints. This in turn is determined by the level of osteotomy and extent of lengthening (3). The knowledge of the muscles’ topography will not only prevent complications like contractures, but also to prevent undue stretching of muscles causing irreversible damage and sharp decline in function (4). Our knowledge of anatomy alerts the following possibilities during lengthening of a long bone.
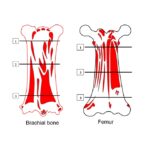
1. If the osteotomy is distal to the muscle insertion, it
remains with the proximal fragment. 2. If the osteotomy is proximal to muscle insertion, the insertion is pulled down as the bone is elongated. 3. If the muscle is attached across a considerable length of the bone, corticotomy can injure the muscle. With subsequent elongation, the muscle bundles attached to the bone also moves expanding its attachment to the regenerate bone. 4. With multilevel corticotomy and polyfocal lengthening of a single bone, a combination of the above occurs. 5. There is another group of biarticular muscles span the joint above and below the bone and lengthen by their whole length irrespective of the level of osteotomy.
Considering that there are at least 20 muscles regulating the function of knee and ankle, a knowledge of muscle that topography becomes mandatory to the limb lengthening surgeon to maintain optimum limb function after tibial lengthening. We propose a simple and practical nomenclature system to simplify the effect of limb lengthening on the muscles and
Corresponding Author: Koushik Narayan Subramanyam, Department of Orthopaedics, Sri Sathya Sai Institute of Higher Medical Sciences – Prashanthigram, Puttaparthi, Andhra Pradesh, India
Email: drkoushik@hotmail.com
Arch Bone Jt Surg. 2018; 6(4): 331-334.
the online version of this article abjs.mums.ac.ir
THE ARCHIVES OF BONE AND JOINT SURGERY. ABJS.MUMS.AC.IR
VOLUME 6. NUMBER 4. JULY 2018
Myotopography in Ilizarov
demonstrate it in the scenario of tibial lengthening.
Technical note
After reviewing anatomical atlases and verifying in cadaveric specimens, we created a universal nomenclature system of muscles and applied it in the leg segment. The purpose of the proposed classification system of muscles is to briefly and visually characterize each muscle participating in lengthening of this segment in terms of the consequences for both the muscle itself and changes in the biomechanical conditions of its operation. The coding of muscles is designed so that it would be possible, without referring to any literature or atlases, to clarify the anatomy and topography of a particular muscle, and also to understand the nature of its involvement in lengthening the tibia.
The composition of the encoding is a matrix of 9 characters, divided into three groups, which are separated from one another by a hyphen (-). In each group there are three items, which are separated by a dot (.) For ease of communication let us represent it as
1.2.3 – 4.5.6 – 7.8.9 and explain what each unit means. Position 1 reflects to which limb segment the given muscle belongs. It can be anything of trunk (Tr), arm (Br), forearm (An), hand (Mn), pelvis (Pl), thigh (Fm), leg (Cr), leg (Cr) and foot (Pd), as derived from their Latin equivalents – Trunk, Brachii, Antebrachii, Manus, Pelvis, Femoris, Cruris and Pedis. Position 2 shows how many joints are affected by the action of this muscle. The possible values are: 1 – for uniarticluar muscles and 2 – for biarticular muscles. Positon 3 is a three- digit number that expresses the possibility of injury to the muscle during corticotomy of the long bone at various levels as explained in Table 1.
Position 4 reflects the proximal level of attachment of the muscle according to the abbreviations proposed for position 1 (Tr, Br, An, Mn, Pl, Fm, Cr, Pd). For muscles around the knee and ankle, it gets a value of Pl or Fm if the muscle origin in above knee and 0 if muscle origin in below knee. Position 5 gets Cr for origins from leg segment and Fm or Cr insertion of uniarticular muscles and 0 for biarticular muscles. Position 6 denotes insertion of uniarticular muscles originating below
knee and bi-articular muscles.
Positions 7, 8 and 9 correspond to upper middle and lower third of corticotomy respectively. Values here show whether the muscle is stretched when bone is lengthened by a corticotomy at this level. The possible values for each are: 0 – does not stretch and 1 – stretches with distraction.
To demonstrate one example, let us take the muscle Articularis genus. The nomenclature looks like: Fm.1.000
– Fm.Cr.0 – 0.0.0. This record informs us that this muscle belongs to the thigh muscles (Fm), uniarticluar (1), not injured in osteotomy of tibia at any level (000), takes origin in thigh segment and is attached to leg segment (Fm.Cr. 0), does not stretch with distraction of tibial corticotomy at any level (0.0.0.). This encoding system is an easily readable and compact way of recording a significant amount of information about the muscle for practical use in planning the surgical intervention. Accordingly all the muscles involved in tibial lengthening are encoded in Table 2.
Discussion
It is well known that limb lengthening causes pain and stiffness of adjacent joints (4). Monofocal lengthening at the rate of 1mm per day is believed to be the most optimum (5). However this is time consuming. Bifocal lengthening apepars to reduce total treatment time (4). By performing simultaneous distraction at two osteotomy sites in the same bone segment, total daily lengthening is increased and length is achieved in a shorter time. This based on the assumption that both osteogenesis and soft tissue adaptation across one osteotomy take place independently of the simultaneous distraction at the other site. Problems arise when this soft tissue adaptation lags the extent of bone lengthening (4).
Current evidence says that elongation of the muscle occurs throughout the muscle substance, and not only at the osteotomy site. Consequently, the load on the soft tissues depends not only on the distraction rate at the nearest osteotomy site, but also on the total daily lengthening of the bone segment and resistance to distraction is contributed by soft tissue and not by the regenerate bone (7).
| Table 1. Possible values at positon 3 of the proposed topographic nomenclature based on possibility of muscle injury during corticotomy at different locations of the bone | |
| Value | Interpreting a symbol |
| 000 | Muscle is not injured irrespective of level of corticotomy |
| 100 | Muscle is injured during corticitomy at upper third of the long bone |
| 110 | Muscle is damaged during corticotomy at the upper and middle third of the long bone |
| 010 | Muscle is damaged during corticotomy at the middle third of the long bone |
| 011 | Muscle is damaged during corticotomy at the middle and lower third of this segment |
| 001 | The muscle is damaged during corticotomy only in the lower third of the long bone |
| 111 | Muscle is damaged during corticotomy at any of the three levels |
THE ARCHIVES OF BONE AND JOINT SURGERY. ABJS.MUMS.AC.IR
VOLUME 6. NUMBER 4. JULY 2018
Myotopography in Ilizarov
| Table 2. Systematic codified nomenclature of muscles involved in tibial lengthening based on their susceptibility to injury and stretch. | ||
| Name of the muscle | Coding of muscle | |
| Muscles that don’t get injured but lengthen irrespective of the level of corticotomy (biarticluar) | ||
| 1 | Plantaris | (Cr.2.000 – Fm.0.Pd – 1.1.1) |
| 2 | Gastrocnemius | (Cr.2.000 – Fm.0.Pd – 1.1.1) |
| Muscles that don’t get injured or elongate irrespective of level of tibial cortictoomy | ||
| 3 | Articularis genus | (Fm.1.000 – Fm.Cr.0 – 0.0.0) |
| 4 | Biceps femoris | (Fm.1.000 – Fm.Cr.0 – 0.0.0) |
| 5 | Quadriceps femoris | (Fm.1.000 – Fm.Cr.0 – 0.0.0) |
| 6 | Semitendinosus | (Fm.2.000 – Pl.0. Cr – 0.0.0) |
| 7 | Semimembranosus | (Fm.2.000 – Pl.0. Cr – 0.0.0) |
| 8 | Rectus femoris (quadriceps femoris) | (Fm.2.000 – Pl.0. Cr – 0.0.0) |
| 9 | Gracilis | (Fm.2.000 – Pl.0. Cr – 0.0.0) |
| 10 | Sartorius | (Fm.2.000 – Pl.0. Cr – 0.0.0) |
| 11 | Popliteus | (Cr.1.100 – Fm.Cr.0 – 0.0.0) |
| Muscles that get injured or stretched depending on the level of corticitomy and lengthening | ||
| 12 | Flехоr digitorum longus | (Cr.1. 010 – 0.Cr.Pd – 0.1.1) |
| 13 | Flexor hallucis longus | (Cr.1. 010 – 0.Cr.Pd – 0.1.1) |
| 14 | Tibialis posterior | (Cr.1. 110 – 0.Cr.Pd – 1.1.1) |
| 15 | Soleus | (Cr.1.110 – 0.Cr.Pd – 1.1.1) |
| 16 | Peroneus longus | (Cr.1.110 – 0.Cr.Pd – 1.1.1) |
| 17 | Peroneus brevis | (Cr.1.010 – 0.Cr.Pd – 0.1.1) |
| 18 | Tibialis anterior | (Cr.1.110 – 0.Cr.Pd – 1.1.1) |
| 19 | Extensor digitorum longus | (Cr.1.110 – 0.Cr.Pd – 1.1.1) |
| 20 | Extensor hallucis longus | (Cr.1.010 – 0.Cr.Pd – 0.1.1) |
The evolution of such a myotopographical chart has the following clinical implications [Table 2]. Depending on the level and number of osteotomies, as well as the magnitude of lengthening of the bone at each level, different muscles are subjected to stretching to varying degrees (7). A precise knowledge of which all muscles that are affected in these different scenarios is important for the surgeon to monitor for obstacles and complications during lengthening and prevent them. The current scheme summarises every effect that corticotomy and distraction pose on each muscle involved in the segment.
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Informed consent and Ethics committee certification are not applicable for this paper as it is a technical note.
Konstantin Igorevich Novikov PhD Oleg Vladimirovich Klimov MD Andrey Sergeevich Neretin MD Olga Stepanovna Novikova MD
T & O Department, Russian Ilizarov Scientific Centre for Restorative Traumatology and Orthopaedics, Kurgan, Russia
Koushik Narayan Subramanyam MS MRCSEd Department of Orthopaedics, Sri Sathya Sai Institute of Higher Medical Sciences, Prashanthigram, Puttaparthi, Andhra Pradesh, India
These observations must be validated with cadaveric experiments. Sonographical assessment will further help to confirm the muscles affected in each of these scenarios and also tell the extent of injury according to the degree of lengthening. The scheme presented above reiterates the fact that limb lengthening is not just confined to bone, but also extends to soft tissues that may sometimes be more limiting and less forgiving than bone itself.
THE ARCHIVES OF BONE AND JOINT SURGERY. ABJS.MUMS.AC.IR
VOLUME 6. NUMBER 4. JULY 2018
Myotopography in Ilizarov
References
- Aslani H, Tabrizi A, Sadighi A, Mirbolook AR. Treatment of pediatric open femoral fractures with external fixator versus flexible intramedullary nails. Arch Bone Jt Surg. 2013; 1(2):64-7.
- Novikov KI, Subramanyam KN, Kolesnikov SV, Chegurov OK. Kolesnikova ES. Mundargi AV. Ilizarov stump lenthening can aggravate phantom limb pain
– a case report. Arch Bone Jt Surg. 2018; 6(3):240-2.
- Thorey F, Bruenger J, Windhagen H, Witte F. Muscle response to leg lengthening during distraction osteogenesis. J Orthop Res. 2009; 27(4):483-8.
- Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin
Orthop Relat Res. 1990; 250(1):81–104.
- Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res. 1989; 239:263-85.
- Choi IH, Sohn CS, Chung CY, Cho TJ, Lee JW, Lee DY. Optimum ratio of distraction in double level tibial lengthening. Clin Orthop Relat Res. 1999; 368:240-6.
- Aarnes GT, Steen H, Kristiansen LP, Ludvigsen P, Reikerås O.Tissue response during monofocal and bifocal leg lengthening in patients. J Orthop Res. 2002; 20(1):137–41.